
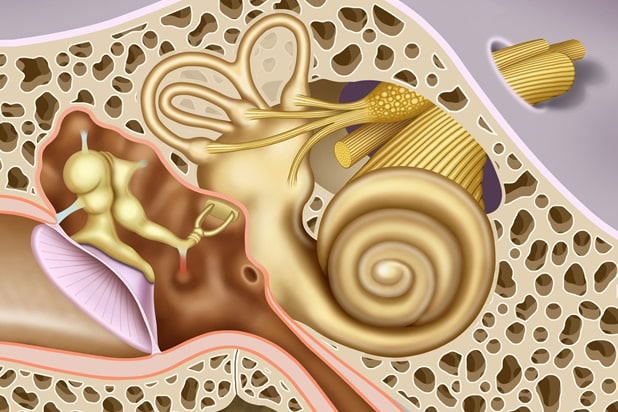
The cochlear (hearing) nerve
Acoustic Neuroma most commonly arise from nerve sheath cells in the vestibular nerve portion of the vestibulocochlear (CN 8) nerve. Because the tumor does not arise from the cochlear nerve itself, patients with smaller Acoustic Neuroma can present with significant dizziness and balance difficulty and can still retain much of their hearing. At The Center for Acoustic Neuroma, we favor a hearing preservation treatment approach for patients with good hearing (speech discrimination above 70% by audiogram) and tumors smaller than 2.5 cm. Maximal attention still has to be paid to the facial nerve during resection of these tumors.
Much of the evaluation of a patient with Acoustic Neuroma is spent not only characterizing the tumor but also considering the impact of the tumor on the individual’s life. Patients that have intact hearing and a smaller tumor may consider surgical options for removal of the tumor while maintaining the hearing nerve and long term hearing. Often we will obtain an auditory brainstem response (ABR) test before the surgery to assess how hearing information is travelling across the nerve.
If a hearing preservation middle fossa or retrosigmoid approach is considered, it is advantageous to proceed with this surgery while the tumor is small and while the patient has retained as much hearing as possible. In these cases, we often will counsel the patient that removing the tumor sooner after diagnosis is preferable so that we may give individuals the best chance of retaining their hearing.
We monitor the sound transmission across the cochlear nerve during any hearing preservation surgery using real time Auditory Brainstem Response (ABR), or Brainstem Auditory Evoked Response, testing. This allows us to track the hearing during resection of the tumor.